At our last allergist visit, they ran the numbers on a number of varieties of beans and many were Class 0, with values like 0.68. My son's doctor thought it was reasonable to try these at home.

He has avoided all beans since around age five, when he started developing new allergies. First it was tuna. Then cashews. Then (to our great surprise), he suddenly became allergic to garbonzo beans, something he had eaten very regularly through toddlerhood. Then it was sugar snap peas. Green beans. Baked beans (a particularly scary reaction that happened at his aunt's house, out of town, without medication in hand). The doctor actually thought it was possible he had something called "idiopathic anaphylaxis" at the time - reactions from unknown causes. However, after we kept a careful journal and did some testing and even in-office challenges, it became apparent he had developed a bean allergy.
At that point, we just started avoiding all beans and peas, which our doctor thought was reasonable. It turns out that 1 in 20 kids can have an allergy to a seed protein that's shared between bean species. If my son had that type of allergy, it was possible even more bean sensitivities would surface.
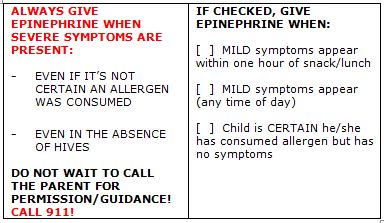
We followed the same protocol as in the office: start with 1/4 of a bean and double the amount every 20 minutes until he reaches several Tbsps. of the food. The hardest part is that he has to discontinue his antihistamine for 7 days before.
We introduced kidney beans and my son had no problem during the challenge. However, the next day, he threw up after eating chili with kidney beans. A couple days following - exact same result. We all sighed and put it back on the list of foods to avoid.
This time, thankfully, things were different. Both pinto beans and cannillini beans went off without a hitch.
Did my son really outgrow beans this time? Might the FAHF-2 have helped? Or were we just avoiding two varieties that he could have tolerated all along? We don't know.
It's also early days with beans. We could have the same experience as several years back, where he succeeded in the challenge but really can't tolerate beans in his diet.
My husband had a gleam in his eye last night. He said to me for the first time "do you ever wonder if he's just not allergic to anything any more except peanut?" Yes, I wonder. It's time to do an open milk challenge and find out.

Yes, I'm grateful. Happy Thanksgiving to all of you celebrating this week!
Follow me on Facebook or Twitter


































.jpg/320px-Children_about_to_board_the_school_bus_(Thibodaux,_Louisiana).jpg)